


When it comes to hormone imbalances in Prader-Willi syndrome (PWS), growth hormone deficiency and growth hormone therapy are at the forefront of the conversation. However, the levels of several other hormones are also more frequently different in PWS as compared to the general population. Data from the Global PWS Registry shows that 20% report having a thyroid issue. The prevalence increases with age, with 15% of participants under the age of 5 reporting a thyroid issue, while 24% of participants over the age of 21 report thyroid problems.
Impact of Thyroid Hormone Levels
There are conflicting reports in the medical literature about the incidence of low thyroid hormone levels (hypothyroidism) in PWS. Thyroid hormones help regulate metabolism, and so are an important part of overall clinical care and management in PWS. Low levels of thyroid hormone can lead to a variety of symptoms including weight gain, lack of energy, hair loss, constipation, and depression. Long term untreated hypothyroidism can cause intellectual disability and nerve damage. Considering that many of these symptoms are already associated with PWS, hypothyroidism in a person with PWS could contribute to worsening some of these symptoms.
Registry Data on Thyroid Issues In PWS
Some studies report that the incidence of hypothyroidism in PWS is the same as in the general population (~2%). However, there are also studies that report a higher frequency of hypothyroidism in PWS. Here, we report the findings from the Global PWS Registry. Over 700 participants have completed the Endocrinology Survey within the Registry, and overall 20% report having a thyroid issue. The prevalence increases with age, with 15% of participants under the age of 5 reporting a thyroid issue, while 24% of participants over the age of 21 report thyroid problems.
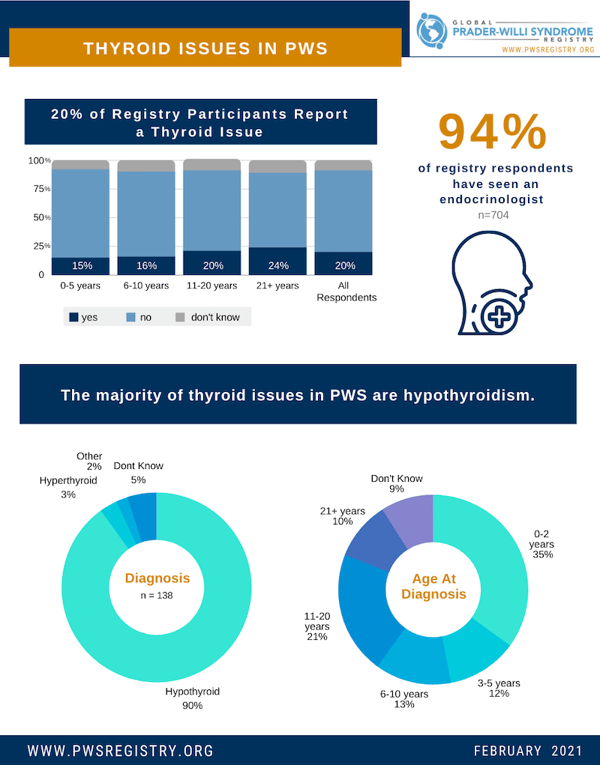
Of participants in the Registry who report a thyroid issue, the vast majority (90%) are hypothyroidism, or low thyroid levels. It is important to note that there are different types of hypothyroidism based on the biological reason for the thyroid hormone deficiency. Thyroid hormones are made and released by the thyroid gland. In some cases the thyroid gland itself is physically attacked and destroyed by a person’s immune system (primary hypothyroidism due to autoimmunity). In other cases, the thyroid gland is intact, but the signals that tell the gland to produce thyroid hormones are not working correctly (secondary or central hypothyroidism). The Endocrinology Survey in the Registry does not currently ask participants to distinguish the type of hypothyroidism they have, but other studies have shown that most people with PWS and hypothyroidism have secondary or central hypothyroidism. Although the underlying cause may vary, treatment is generally the same, consisting of a daily medication to replace the missing hormone.
For Registry participants with a thyroid issue, almost half (47%) were diagnosed before the age of 5 years old. However, 10% of individuals were diagnosed as adults over the age of 21, indicating the importance of monitoring thyroid function in people with PWS from infancy through adulthood. Fortunately, a simple blood test can detect hypothyroidism, and the treatment is quite effective.
For more information on the Global PWS Registry, please visit pwsregistry.org or email the Registry here.



