


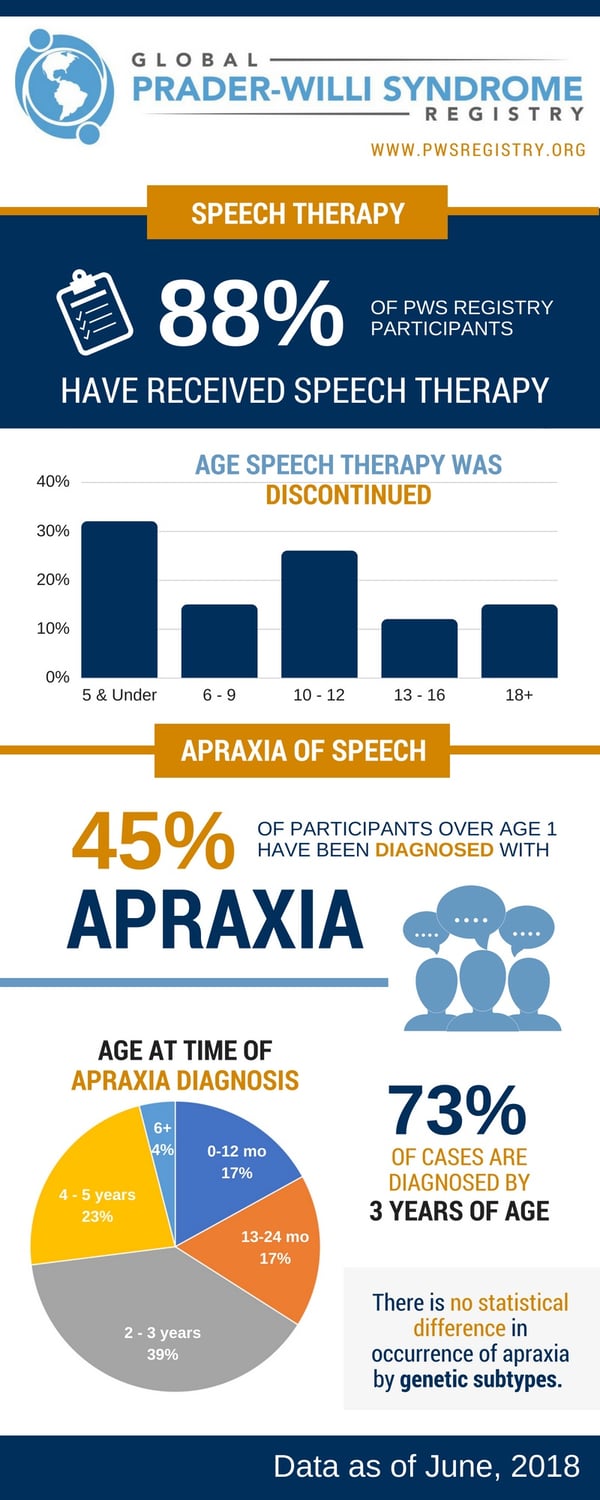
Speech requires a complex combination of cognitive processing to quickly find and combine the right words, paired with the physical process of producing sounds. Since PWS impacts a variety of pathways that contribute to speech and sound development, it is not surprising that 88% of individuals within the Global PWS Registry have at some point received speech therapy. The factors affecting speech and communication in PWS include issues with developmental delays, auditory and cognitive processing, oral and facial muscle strength, high-arched palate, and low saliva production. With regard to the sounds of speech in PWS, characteristics often include unusual prosody, or melody of speech; difficulty with articulating words; hypernasality; a slow speaking rate; and flat or abnormal pitch and intonation.
One of the most frustrating impacts to speech and sound development in PWS is childhood apraxia of speech (AOS). In individuals with childhood AOS, there is a disconnect between the brain and the physical processes required for speech. S/he knows what s/he wants to say, but has difficulty with motor programming, the actual process of making the correct sequence of movements to produce the right sounds. Symptoms can include things like distorting words or sounds, difficulty repeating words or sounds, and physically groping for the correct word. This is different than a developmental language delay where there are deficits or delays in learning words and language. In fact, some individuals with PWS may have both childhood AOS and delayed language development.
Within the Global PWS Registry, 45% of the participants over age 1 have been diagnosed with childhood AOS. For the majority of individuals, the age of diagnosis is between 2-5 years old (62%). It is important to note that although 34% of participants report receiving a diagnosis before age 2, there is debate and controversy within the field of speech and language pathology as to whether a formal diagnosis of childhood AOS can be made that young.
An important "take-away" from the data on speech problems in the PWS Registry is that one of the important things to consider shortly after diagnosis of PWS is a consultation with a speech language pathologist (SLP). This type of professional can help with feeding and oral motor skills early on, as well as monitor for speech and language development, and provide speech therapy if needed. For those with a diagnosis of childhood AOS, incorporating alternative communication strategies such as sign language and picture boards can help alleviate some of the associated frustration associated while oral skills are developing. There are also groups dedicated to childhood AOS, including Apraxia-Kids and Let’s Talk Apraxia.
In the four-minute video below, Dr. Edythe Strand, Emeritus Professor and Consultant, division of Speech Pathology, Department of Neurology, Mayo Clinic, provides a complete description of CAS. The nature of the neurologic deficits that may be involved are discussed, and terms related to CAS such as planning and programming for speech and proprioception are described.



